Question - What are the various thresholds?
- What is a threshold? Why measure thresholds?
- The term threshold has many meanings. The simple definition in common usage is any place or point of entering or beginning something, for example, the threshold to a house is the doorway, marriage is a threshold to a new way of life. In medicine or biology it has the meaning of the place or point of beginning; the lowest point at which a stimulus begins to produce a sensation; or the minimal stimulus that produces excitation of any structure, eliciting a motor or chemical response.
Thresholds are important in exercise physiology because something different biologically happens at a certain effort level. Very often these thresholds correlate with performance in athletic events. Thus, knowing these thresholds will indicate how well the athlete will do in a competition and how the athlete has responded to training. They can be a measure of how effective the training has been. This series of questions is focused on thresholds that have to do with lactate, directly or indirectly. There are other thresholds using other measures, but nearly all these thresholds correlate highly with the lactate thresholds discussed here.
Despite lots of different names, there are really only two thresholds that have been identified in the literature and only one of them is meaningful.
- What is the anaerobic threshold?
- The anaerobic threshold is a term coined in 1964 by Karl Wasserman when he used V02 measurements to show a change in the gas curve that seemed to correspond with an increase in lactate in the blood. At a point on the gas curve, C02 increased more than he expected. The subjects were producing more lactate than the muscles could consume; the buffering of this lactate was thought to cause the observed increase in C02. Wasserman called this the anaerobic threshold because it was thought that the body was suddenly transitioning to anaerobic metabolism.
Wasserman, K. and M. B. McIlroy (1964). "Detecting the threshold of anaerobic metabolism in cardiac patients during exercise." American Journal of Cardiology 14(6): 844-852.
Some other researchers later pointed out that while excess lactate was being produced and it appeared in the blood stream, the body was still in a steady state. Oxygen was still being used in ever greater amounts and there was no sudden change to another energy system. So while the lactate in the blood indicated a somewhat greater involvement of the anaerobic system, and C02 increased confirming this, aerobic metabolism was still the main source of energy, was still increasing and was not near maximum.
(It should be noted that the term anaerobic threshold has in recent years been re-defined to mean a much higher effort level: the maximum level that an athlete can maintain for a long time without causing lactate to rise sharply.) See What is the lactate threshold? just below.
- More on the Wasserman Study
- Here are two quotes from the original Wasserman study. First,
The onset of anaerobic metabolism during exercise can thus be detected in three ways: (1) as an increase in the lactate concentration in blood, (2) as a decrease in arterial blood bicarbonate and pH and (3) as an increase in the respiratory gas exchange ratio (R).
and second,
Thus, it is possible for the examiner to detect the threshold of anaerobic metabolism during the work test
He then went on and used the specific term, "anaerobic threshold" because he believed that this was where the anaerobic system took over. He was wrong about this and that is what science is about. Discoveries like Wasserman's are what move the ball along but unfortunately his idea of a major abrupt change in anaerobic metabolism was wrong. This misconception persists till today with many people. Anaerobic metabolism occurs before this so-called threshold point, and aerobic metabolism continues after it. And the place on the gas curve he pointed out is not an important point for training for endurance sports. Wasserman was not the first to find this point: Hollmann had published the same information in 1959, but Hollmann’s work was in German and not known in most of the world at that time. Both Hollmann and Wasserman are still alive in 2015. Hollmann was head of the German Sports Academy where Alois Mader worked and Jan Olbrecht got his degree. And who are these people? They figured out how the body mixes aerobic and anaerobic metabolism and how to use this information to train athletes. There is more information about them and their discoveries below. We also have a more detailed discussion on this topic on our thresholds page especially on how to train the thresholds. But before you do that, you should read about the term, lactate threshold
Return to Questions Page
- What is the lactate threshold?
- Originally what was called the anaerobic threshold point coincided exactly or approximately with the point where blood lactate rose over baseline levels. Other researchers then re-named this point where the lactate rises, as the "lactate threshold". In fact there is no real threshold here, nor has any real transition taken place; still, two different researchers used the term “threshold” for these points.
The curve below is a typical lactate curve. Several measurements have been taken as well as a resting lactate. Notice that the lactate remains close to the resting rate for several measurements even though the muscles are producing anaerobic energy, and producing pyruvate and lactate. When the lactate starts to rise, this means some of the lactate being produced is entering the bloodstream where it is being measured. It is hard to pinpoint a specific place on the curve where the rise really starts. There are no gas measurements here so there are no V02 and C02 measurements to find the ventilatory threshold, which is what the original anaerobic threshold is now called. We will ask a question of the reader: where does the lactate curve start to rise? The problem with getting an acceptable answer to this question has taken up a lot of the time of many researchers. We will take the point of view that the answer doesn't matter, even if there is a correct one. So the athlete should not worry about it.
An athlete could continue to increase his intensity above this point where the curve starts to rise and still be in a steady state in terms of lactate in the blood. A steady state means that if the athlete continues at that pace, most physiological measures will remain constant. Lactate, oxygen consumption, heart rate, perceived exertion will stay fairly constant just at slightly higher level. At 9 mph, this athlete’s lactate is now a little higher, but it is still in a steady state: he can maintain this pace for a long time without his lactate changing.
At some point for every athlete, there is a higher effort level, where lactate is no longer in a steady state. Trying to continue indefinitely at this pace will not be possible: lactate rises sharply and the athlete has to stop. This truly represents a transition where the muscles eventually have to cease contraction – a true threshold. So this higher level became known as the anaerobic threshold even though Wassermann had named the lower effort level where lactate first starts to rise, the anaerobic threshold. The earlier concept was re-named the aerobic threshold by some, though there is no reason why it should be designated as aerobic. Aerobic metabolism does not stop there, nor does it begin there, nor does it change in any significant way there. The common name for this lower level when it is determined by gas measurements is the ventilatory threshold.
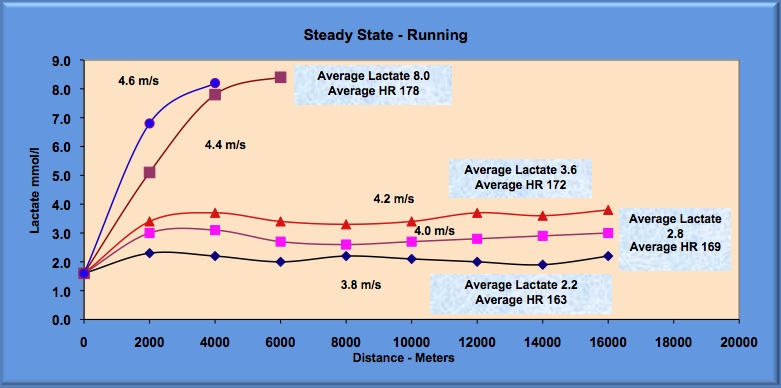
Beyond the higher level, lactate increases steadily, so this higher level is more appropriately referred to as the lactate threshold (even though this had also been used for the lower level). Since this was the effort level most useful in predicting performance, this term stuck, at least to the present time. Most people use the term lactate threshold to mean the second and higher level while academics use lactate threshold to mean the lower level. This terminology is a mess since most people use the term anaerobic threshold and lactate threshold to mean the same thing, and it is different from the original use. Most use it for the higher point, which is a true transition but as I said, academics don't. Below is a set of curves depicting steady-state runs and two after the runner reaches a point where the runs are no longer steady-state.
In the spirit of compromise some researchers want to use the term "lactate threshold" to mean two things, the lower level and the higher level. They want to rename these points Lactate Thresholdaerobic and Lactate Thresholdanaerobic They want to call the range in between the two points the aerobic-anaerobic transition. Unfortunately none of these terms makes sense. There is only one transition and that is at the higher effort point. The transition has nothing to do with any changes to or from aerobic or anaerobic metabolism. At both points, the lower point and the higher point, there is a gradual increase in both energy systems and neither point has anything to do with training effects. The transition at the higher level has to do with the capacity of the cells to utilize lactate as a fuel versus the rate at which it is being produced. It has nothing to do with one system producing more and the other system producing less or even staying still. Both are increasing at the threshold. It is more like a pump in your basement trying to empty water that is coming in due to heavy rains. If the rains are too heavy, eventually the best pump will be overwhelmed and the basement will flood. So the transition at the higher threshold has more to do with the relative strength of the two energy systems than any transition of either one to some new state.
The water in the basement analogy is a great way to understand the lactate threshold. If it stops raining or slows to a drizzle, the level of the water in the basement will go down. This is equivalent to less lactate production. If the pump is much stronger than even a large amount of water can be eliminated and the level of water will go down. This is equivalent to having a large aerobic system which will eliminate the lactate. Most of the lactate is being eliminated by the strong aerobic system..
At both points, the lower point and the higher point, aerobic and anaerobic energy are increasing. There is no transition to a new source of energy other than each is getting a little bit higher. Using terminology that implies that there is some change going on in either system has only led to confusion. We have a more detailed discussion on this topic on our lactate threshold page and thresholds page especially on how to train the thresholds.
Return to Questions Page
- What happens because lactate continually increases above the lactate threshold. Why is "lactate threshold" the best name for what happens at this higher turn point of the lactate curve?
- Lactate itself does not cause the problem. That should be emphasized. But because it is not being eliminated or utilized as it is produced all sorts of negative things do happen. When we say it is being eliminated, we really mean that it is being used as fuel for the aerobic system. When lactate is eliminated/utilizied it produces ATP. This process takes a phosphate ion in the muscles and recombines it with ADP to produce ATP the basic molecule for energy contraction. If the lactate cannot be utilized/eliminated phosphate ions (Pi) will start to accumulate in the muscles.
When lactate is eliminated/utilized, it will also remove hydorgen ions produced during glycolysis from the muscle cell. So when lactate is not eliminated hydrogen ions will start accumulating and the Ph of the cell will drop to levels, sometimes to levels that might be dangerous. And it can do it extremely quickly if the effort level is very high.
Because the muscle needs a high level of energy to continue contracting at these high effort levles, it will look for other ways to combine the Pi or phosphate ion with ADP to make ATP. The only available system to do this is the creatine phosphate system. This will drive PCr (creatine phosphate) even lower and when it reaches a certain the point the muscles must stop contracting.
All becasue lactate is not being utilized. So the effort level at which this happens is best described as the
"lactate threshold."
- One might ask, which is the easiest of all these lactate tests? (see previous question above)
- We haven't a clue how to do the LT Log test and we have been involved in lactate testing for 20 years. We suspect that few coaches would know either. It is basically an exercise for academics and has little relevance for training athletes. The LT baseline is a relatively easy approach. Here is an example of a test done on a college soccer player. But then again, it may be difficult to pinpoint the exact place where the curve begins to rise.
And there are times when it is difficult to measure a baseline. For example, where is the baseline on the following lactate curve? This curve would also cause a problem for those using the LT 1 mmol/l approach. Picking the point becomes a little bit arbitrary. It would also cause problems for those using the two Dmax approaches. The easiest test of all is the L4 or what we call the V4 which also has a high correlation with performance.
There have been several other studies that have showed the predictive power of a simple lactate test for performance. The longer the distance the higher the correlation between the lactate test and competition times. It is interesting that in order to avoid a lactate test, most cyclists will do an all out one hour time trial that is very difficult to complete and which requires a strong motivation. Why would anyone do this when a simple 6 minute sub-maximal test tells the coach or athlete the same thing?
For shorter distances the prediction is still good but less because the anaerobic system becomes more important. So lactate tests of the anaerobic system become more predictive of success.
- Are their other thresholds? What are their names?
- There are several other names for thresholds. We will examine a few here. Most are just a different name for the two thresholds we just considered.
Return to Questions Page
- What is OBLA?
- In the early 1970's Alois Mader was working with East German runners. He found that a high percentage of these runners could run at a pace that generated 4 mmol/l of lactate for a long time but not at any higher level. He pointed to this 4 mmol/l as an important marker of an athlete's conditioning. When Mader escaped to the West, he went to the Sports School at Cologne and popularized the 4 mmol/l measure.
Early on several sports scientists experimented with the 4 mmol/l level and the training of athletes. Two, Bertil Sjödin, from Sweden, and Ira Jacobs, a Canadian graduate student working with Sjödin, did some studies on the correlation between the pace at 4 mmol/l and running performance and published their results starting in 1981. The title of the first article they wrote was "Onset of Blood Lactate Accumulation and Marathon Running Performance." This quickly became OBLA. Since that time the 4mmol/l level has been associated with OBLA as well as the anaerobic threshold. Before then in 1979 in an article by Farrell and several others, these researchers used the term Onset of Plasma Lactate. They were trying to identify the place where lactate increases exponentially in plasma or essentially they were trying to find the point of maximum sustained effort where lactate remained constant.
And this is just the beginning of the confusion. Today, OBLA is a moderately searched term in google which means that some athletes still hear it. And 4.0 mmol/l of lactate is still a commonly used variable in the assessment of an athlete's conditioning. We will discuss this more below. And many researchers are using OBLA to mean the maximal lactate steady state which is what the original intent of the term was. And a few are using it to mean where the blood first starts to rise over baseline or near 2 mmol/l.
- What is IAT or the Individual Anaerobic Threshold?
- Three German sports scientists in 1981 showed that the lactate levels at this maximum steady state varied substantially and frequently were below 4 mmol/l and sometimes higher. They developed a test to find this individual level and called it the Individual Anaerobic Threshold. (Stegmann H., Kindermann W., Schnabel A: Lactate kinetics and individual anaerobic threshold.) Notice that the anaerobic threshold which was originally associated with an initial rise of lactate above baseline at a lactate level that was probably near 2 mmol/l for most people was raised to 4.0 mmol/l by Mader and now is for most athletes somewhere in between these two points. Confusing, you bet. We are far from done with confusion, because enter a new term that perhaps makes more sense. It is the Maximal Lactate Steady State or MaxLass or MLSS
- What is the maximal lactate steady state?
- We do not know who first named this term. In 1966 a German sports scientist Joseph Keul used the term maximal steady state but in German. In 1975 an American, Londeree used the term maximal steady state in the title of an article. In 1981 another American, Lafontaine showed that for male runners the pace that produce 2.2 mmol/l of lactate on a treadmill correlated extremely high with the pace used to complete a 8 km run. Similar to what the OBLA people had shown but using 2.2 mmol/ instead of 4 mmol/l. Lafontaine called the lactate level the maximal steady state implying that it was the highest steady state for which lactate remained constant. In 1982 in an article by Stegmann and Kindermann, they used the term "maximal lactate steady state." That is the earliest that we have found the term used in any literature. If any reader knows of an earlier use of this term, let us know.
The maximal lactate steady state or MaxLass or MLSS is the term of choice to indicate the effort level where a real transition takes place. Above this pace, lactate will accumulate rapidly in the muscle and blood. Eventually the muscles affected will not be able to contract. When this happens the athlete will often adjust by using awkward movement, essentially using other muscles, to finish a race. It is not uncommon to see a swimmer's perfect stroke break down a few meters from the finish. The swimmer will continue on for the final few seconds by adjusting his or her stroke thereby using muscles to finish the race that are not shut down by acidosis. You also often see this in running races especially those from 800 m to 3000 m when the runner's normal stride falls apart. In the above chart on steady state runs the maximal lactate steady state is somewhat above 4.2 m/s and below 4.4 m/s. To find the exact spot is painstaking and, we believe, not worth it. It is of interest to researchers but it is not necessary to know it to train wisely.
We have just said that the maximal lactate steady state is the only valid point where there is a real transition or threshold, but that it is not worth measuring. First, of all it is certainly worth the effort for researchers to measure it because it will be a variable in their work that should be accounted for. But for a coach or athlete, it is probably a waste of time. There are other measures much more easily done that correlate almost perfectly with MLSS. And there is no need to train at or near the MLSS because it is too intensive for most athletes to handle, especially elite athletes. So for a coach it is expedient to use these other easier methods. And what is another measure? We recommend that the most useful measure is the pace or effort at 4 mmol/l.
Return to Questions Page
- So the best measure for lactate testing is the one that most say is meaningless?
- We have had many conversations with respected researchers in exercise physiology who have told us it is a complete waste of time to measure the 4 mmol/l level because it has been completely discredited years ago. We say we understand this but the more sophisticated point of view is to measure it and forget about attempts to measure the lactate threshold or MLSS. This sounds like heresy to these researchers some of whom have invested a lot of time in using various methods to estimate the MLSS. We counter that there is an even more sophisticated way of looking at lactate testing than they are using. This often does not make too many friends but we have found that many of the coaches understand what we are doing when it is explained to them and that the ideas of Mader and Olbrecht coincide more with the views they have for training their athletes.
- Why is 4 mmol/l the best measure for lactate testing?
- First, it is not the best measure but it sure is an easy one to find and use. Look at the curve we presented above. It is presented again here for convenience. Is it difficult to find the point where the lactate is 4 mmol/l?
The 4 mmol/l pace or effort level is easy to find. And 4 mmol/l correlates with performance for most endurance athletes. You do not want to train at the 4 mmol/l pace so if someone is planning training zones it is just as easy to do it with this measure. See the triathlon assessment section for some ideas. And over time the 4 mmol/l represents a measure to evaluate the progress of an athlete. Here is one from a world-class rower. There is an interesting story that goes with this rower concerning training and is on another part of our web site.
There is obviously a bad reading in the above chart. On the blue line at 300 watts, the reading is probably too high. We have used this chart for a couple reasons, one to show the quick change in an athlete's threshold and secondly that some readings may reflect some contamination. If one is using a portable lactate analyzer, it is easy to take a second reading if the first reading appears to be contaminated by sweat or something else. Currently the analyzers provide a reading in 10-13 seconds.
What we are recommending is not 4.0 mmol/l specifically but a fixed level that is easy to measure. We were once at a sports medicine conference in Barbados and some Cuban sports scientists were there. They worked mostly with runners and used a 3 mmol/l level instead. It was closer to the threshold for most of their runners. The reason why we recommend 4 mmol/l is that is nearly always on the upswing of the curve and easy to identify. Too much higher and it is getting out of the range of what the threshold could be and too low and it might be too close to the gently rising part of the curve. It is a good compromise, based on lots of historical data, and it works.
Return to Questions Page
- Some say the threshold exists but do not bother measuring it. Who are they?
- Alois Mader has done more than anyone else to focus attention on lactate testing as a possible way to assess athletic performance. First, In the late 1960's and early 1970's Mader worked for the East German sports machine. He noticed that when his athletes would run at a pace that corresponded to the production of 4 mmol/l of lactate in their blood, they could seemingly run for a long time, and their lactate did not increase above the 4 mmol/l level. When they increased their pace they were forced to stop and the lactate had risen to much higher levels. He then postulated that the anaerobic threshold was 4 mmol/l. When Mader escaped from East Germany and went to The Sports School at Cologne, he published his results and immediately popularized lactate testing as a means of optimizing performance in athletes.
Rivals were quick to point out that the lactate level at which this maximum lactate pace took place varied considerably among individuals from as low as 2.5 mmol/l to as high as 6 or 7 mmol/l and that it varied by sport. See previous question on the Individual Anaerobic Threshold. Also a couple of his students and a local swimming coach went off to conquer the swimming world using the 4 mmol/l concept. And they failed.
Second, but this is where Mader's more important work began. He had been working on a model of energy metabolism and in the mid 1980's he started to publish his results. His findings on how energy metabolism works in humans have largely been ignored. Mader solved the problem as to why the 4 mmol/l measure was limited while developing his model of energy metabolism. The model he developed explains how the muscles decide to produce energy, how much aerobically versus how much anaerobically. He found that the key to energy production was in the strength of the anaerobic system and not just in the aerobic system as most sports physiologists believed at the time. Essentially, Mader showed that the threshold concept of athletic performance was limited and unless a coach considered the anaerobic component, he was missing a key ingredient of performance.
Jan Olbrecht was one of Mader's student's who failed to conquer the swimming world. Jan was a Belgian record holder in freestyle and swam in World Championships. He was very interested in what was behind an athletic performance. He completed his doctorate and validated Mader's ideas for swimming. He has been using them ever since to train athletes and the athletes he helps train have won over 300 Olympic and World Championship medals including the world record holder of the Ironman triathlon for over 15 years. He wrote the book, The Science of Winning, that explains his methods. His ideas form the basis for this web site and most of the CD-ROM, The Secrets of Lactate. The book's focus is on swimming but two top triathlon coaches rate this book as the best book on training for triathletes and it is popular with rowing and skiing coaches as well as swimming coaches. Jan presented at the First World Congress of Science in the Triathlon in Alicante, Spain.
Jan, also minimized the attempt that most sports scientists were pursuing at the time, namely how to measure the threshold. Here is a quote from his book, The Science of Winning:
In the early period of the history of lactate testing it was often suggested that the anaerobic threshold was the optimum training intensity for improving aerobic endurance. Later studies as well as practical experience have shown that this is not the case. Indeed, from the perspective of the physiology and the training science there is very little scientific evidence about the anaerobic threshold being the unique and best intensity for endurance training. The biological adaptations, which are necessary to achieve an improvement in aerobic endurance, are very complex and cannot be generated through one single training intensity. Only a combination of different types of exercises, each of them inducing specific training effects, will improve the swimmer's aerobic conditioning and in the end ensure success in competition.
So, as there is neither scientific nor anecdotal evidence that a training workout at the aerobic or anaerobic threshold has any advantage over a good balanced program of different types of training, the cost in time needed to determine a reliable anaerobic threshold (= the lactate threshold or MaxLass) is not offset. The information gained by the determination of the lactate threshold will not be of any additional help to improve training efficiency. Therefore the determination of an aerobic or anaerobic threshold should be reserved for academic study purposes only.
Moreover, all speculations as well as the lack of a clear statement regarding thresholds provoke with coaches and athletes more confusion than advantages. For this reason we will use the terms fixed aerobic or anaerobic threshold, the individual anaerobic threshold or the lactate steady state as little as possible to avoid the misleading link to the "ideal training intensity".
- What about all those ways people try to measure the lactate threshold?
- On our CD-ROM we discuss several methods people have come up with to measure the lactate threshold. A few years ago a long extensive review of all the ways people have used to measure the threshold was published. It was by Oliver Faude, Wilfried Kindermann and Tim Meyer. Here is the Faude reference and another good one by Ronald Binder and several other authors on the various ways to estimate the threshold.
Faude, O., W. Kindermann, et al. (2009). "Lactate threshold concepts: how valid are they?" Sports Medicine 39(6): 469-90.
Binder, R. K., M. Wonisch, et al. (2008). "Methodological approach to the first and second lactate threshold in incremental cardiopulmonary exercise testing." European Journal of Cardiovascular Prevention & Rehabilitation 15(6): 726-34.
In these two references the controversy over the various uses of the same terms across studies is discussed in detail. It is confusing. We prefer that lactate threshold, anaerobic threshold and maximal lactate steady state be regarded as defining the same phenomenon. We know that this will probably not happen universally in the near term, as many people believe differently. But you should know about the controversy so you are less confused. Here is a blog on rowing that illustrates the confusion. But also remember that there is no value to training at any particular lactate value. That sounds like heresy for people recommending and selling lactate analyzers. But not if you understand the logic of what we are saying.
We mentioned above that there are non lactate thresholds. One frequently used threshold is the ventilatory*. threshold or the VT(sometimes called the GET or gas exchange threshold). This threshold has an interesting history and is what Hollmann and Wasserman actually observed in their original studies. It is not a measure of lactate but of ventilation (VE) or the volume of air exhaled during a VO2 test. At resting levels or low levels of activity the volume of air we breathe in and exhale is the same. The percentage of gases is slightly differnt between what we breathe in and what we exhale. Air is 78% nitrogen and 21% oxygen and carbon dioxide makes a very small part of air, less than 1/10 of a percent. But carbon dioxide makes up about 3% of what we exhale and the amount of oxygen we exhale is less since we use some of it to live.
The total volume we exhale is slightly different from what we inhale but nearly the same.
At a certain point the amount of CO2 we exhale increases more rapidly than the increasse in oxygen we utilize. This causes a non-linear change in the total ventilation (VE) during a graded exercise test. This point seems to occur at the point that lactate rises above baseline levels. So the VT represents some physiological change and it seems to correlate with changes in lactate levels in the blood. That is all we will say about it here but there will be an extensive discussion of this in the near future.
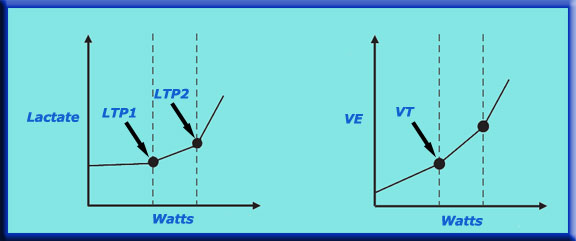
You will notice that in both the lactate curve and VE curves above that there are two places where the curve changes. Many readers will have heard of the first lactate turn point (LTP1) and the second lactate turn point (LTP2). The second lactate turn point is what is known as the maximal lactate steady state and also called the anaerobic threshold and what we prefer to use the term "lactate threshold" for. The first turn point also has many names and we will discuss all these in the future. Some of this is also covered in our thresholds page.
*.Ventilatory means the movement of air so this threshold is about changes in the content of air exhaled over the course of exercise. These changes reflect metabolic processes happening in the body often at the cellular level. Sometimes you will see the term "respiratory" in the context of these discussions. This term means the exchange of one molecule across some kind of membrane in our bodies. Usually it means the exchange of oxygen from one side of a membrane to another. We frequently use the term "respiration" to refer to the uptake of oxygen by the blood in our lungs. It can also mean the uptake of oxygen by the cells especially the mitochondria and oxygen's subsequent use in producing energy.
There are several other non-lactate measures of the two thresholds associated with lactate measures. Most of them are associated with what we call the maximal lactate steady state or lactate threshold. These are critical power (or critical velocity or speed or effort), respiratory compensation point (another ventilation breakpoint), functional threshold (the average power or speed one can hold for an extended period of time, usually greater than 30 minutes but often longer time periods are used), the NIRS-derived deoxygenated hemoglobin(deoxyHbDP) deflection point and the iEMG threshold (integrated Electromyographic) which indicates changes in the EMG signal.
- Will there be more on this topic?
- Of course but this is all for now for this section. Send in your questions and we will try to answer them. We hope to go over all the threshold concepts mentioned in the Faude and Binder articles.
Return to Questions Page